I have had problems with my hip and groin since June. I am hoping to get some advise to supplement the medical advice I have received. I had been working with a PT (He has since moved his office) and massage therapist. Their conclusion is my hip flexor is causing pain in my hip, groin and glute. It is worse 24-36 hours after biking and after any long walks or extended sitting (e.g. long car trips). At the advise of the PT I have stopped running or biking. I did not run much, but was biking 6-8 hours per week. My question is how to strengthen the hip flexor. I have stretches that work well. The PT suggested stabilization by supporting myself while standing on the bad leg. Any thoughts are welcomed.
I have very tight hip flexors and doing skip drills after my runs helps a lot. I do about 10 x 100 meter skips working to get good range of motion. Knee up / Toe up. I do other run drills as well, but the skip drills help the most with my hips. I than stretch a lot. I do a lunge stretch with the front foot on a step or the track stands. I lean into it a good amount until you feel the stretch in the hip of the straight leg. I than follow that up with the thinking man stretch. It’s been about two weeks, since I have been really consistent with it and I have noticed improved ROM and even faster run times during training.
good luck.
jp
Hey Don,
Are you sure that the hip flexor’s weakness is the primary problem? The reason I ask is that typically, the clients I see who have hip flexor pathology are excessively tight through the hip flexor and low back and weak through the abdominal stabilizers and glutes.
While, there’s nothing wrong with working the hip flexor over a full range of motion with a light weight (e.g. standing on one leg away from a cable stack with an ankle cuff on the unsupported leg,& raising the knee toward the chest), I would focus more on dulling down the dominance of the hip-flexors as stabilizers during gait and trying to get the glutes to fire more forcefully. Coupled with low back stretches and a properly designed core program, I think this would be your best route.
Hope this helps.
Alan Couzens, CSCS, PES, ASCA Certified Strength and Conditioning Coach.
Thanks for the feedback. I do have some specific stretches, but this sounds helpful. Don.
Thanks much. I am going back to the gym next week. Your insights are most helpful.
Working the other muscles sounds like the right strategy. The hip flexors are well stretched; and come to think of it, my glutes (right side) get sore after a moderate amount of use. Don.
No Prob Don.
Try some simple cable stuff for the glutes (i.e. side leg raises with your foot slightly behind your body and your toe turned out a little).
It may help if you gently stretch your hip flexor & slowly roll your TFL (the top outside of your thigh) on a foam roll prior to beginning the glute work.
Drop me a line if you need any more info.
Cheers,
Alan
Again thanks Alan. I am working with a trainer, but I think your input will help us both with my leg issue. It has been very frustrating this past season, but I have the winter to get things back so I can train again. I will let you know how it goes. Don.
Hey, while we are talking about the hip, I have a question. I just got diagnosed with tendonitis in my hip :-(, rectus tendonitis (I think that is what it is called). I ran on an off campor road and boom, hosed up hip (okay I ran on it twice). I also realized that my sneakers were a little overdue for a change out. I also had a separated shoulder, which doesn’t really bother me much (cyclocross/pole incident). The doc was more focused on the shoulder so I didn’t get a lot of info on what to do about my hip, except don’t do anything that bothers it. He did say to stretch it. I can cycle/spin but running hurts. What can I do to make it go away faster? I have been behaving and have plenty of time before my first A race (Triple T). Any idea how long it takes to go away? I pretty much stopped running two weeks ago (right after I thought it was tendonitis).
Tamela
First off, let me preface by saying I’m not a PT or an MD.
Short answer is, if it is in the inflammatory stage, I would recommend not stretching it.
As far as the duration of the inflammatory stage, for the lower extremity it can be tough to estimate. Unless you are bed-ridden, you are likely using the hip in your daily activities and if you exceed your pain-free ROM, you risk aggrevating the hip. Take really small steps when you’re walking and avoid any positions that may stretch the hip beyond it’s pain-free ROM.
Obviously, Rest, Ice, Compression, Elevation as much as possible when your resting and some heat in the morning (hot shower, lamp etc) before you begin your day.
I am curious as to the mechanism of your injury. Tendonitis of the rectus femoris muscle would result in pain pretty high up on your ilium (just a little lower than your belly button). I haven’t really seen any clients present with this and can’t think of how running on an off camber road would lead to it. Much more common, from the situation you described, would be ITB tendonitis, trochanteric bursitis or tendonitis of the adducter. Knowing the muscle involved (the weak link) is necessary in determining what rehabilitative exercises should be commenced from here. So I guess the first question is, where does it hurt??
Hope this helps.
Alan Couzens, CSCS, PES, ASCA Strength and Conditioning Coach.
It hurts on the outside of my left hip, right at the hip joint. When I push on it the pain goes away. Right after the initial injury, it hurt to walk for a couple days, now I can feel it, but only hurts if I try to run. Tendonitis just freaks me out because I had it above knee and it took two years to get rid of it (I also ran on it for 6 months before going to the doctor though).
I would suggest going to get a second opinion on the diagnosis. It sounds much more like trochanteric bursitis based on where it hurts.
Check out the symptoms below and see what you think.
www.emedicine.com/pmr/topic141.htm
As far as rehabilitation goes, self myofascial release for the TFL on a foam roll is also appropriate since the TFL is one of those muscles that once it gets inflammed it goes “incredible hulk” on you and wants to exert it’s might in all hip motions. All pain-free hip movements are indicated, especially side lying leg-lifts providing they are pain free.
Hope this helps. Let me know if you need any more info.
Alan Couzens, CSCS, PES, ASCA Strength and Conditioning Coach
Thank you! I read the link, so no compression if it is this? The ortho doc I went to told me he was a hip and shoulder guy, but he put me through a bunch of tests; strength and mobility.
I’ve got something similar and I do a lot of ab/adduction, yoga, get Active Release to separate the inflammation and I also do a drill where I sit back against a wall and raise my leg straight in front of me, hold for 10-20 sec and repeat.
Sorry,
Yeah if it is bursitis, you don’t want to put any pressure on the bursa, as this adds to the inflammation.
Your ortho doc may be spot on, I just haven’t personally seen any cases of tendonitis of the rectus femoris and, knowing the functional anatomy involved, the mechanism, and the point where you feel tenderness, it sounds a lot like some folks I have worked with who have had trochanteric bursitis.
All of that said, if the problem persists, I would definitely get a second op.
All the best for a speedy recovery.
Alan
Hey Don,
Are you sure that the hip flexor’s weakness is the primary problem? The reason I ask is that typically, the clients I see who have hip flexor pathology are excessively tight through the hip flexor and low back and weak through the abdominal stabilizers and glutes.
While, there’s nothing wrong with working the hip flexor over a full range of motion with a light weight (e.g. standing on one leg away from a cable stack with an ankle cuff on the unsupported leg,& raising the knee toward the chest), I would focus more on dulling down the dominance of the hip-flexors as stabilizers during gait and trying to get the glutes to fire more forcefully. Coupled with low back stretches and a properly designed core program, I think this would be your best route.
Hope this helps.
Alan Couzens, CSCS, PES, ASCA Certified Strength and Conditioning Coach.
Alan, I’m just has you described your clients. I have a very tight left hip and sore low back… My hamstrings arn’t bad so I think my gluts are weak. How do I fix this?
Paul
Hey Paul,
There are 2 postural distortion patterns that could come into play here. It’s pretty important to identify which applies to you before proceeding with corrective exercise.
The most important determining factor is the tilt of the pelvis. A simple test is to stand against a wall with your heels flush against the wall. Put your hand in the arch of our back. If you are excessively lordotic (anterior pelvic tilt), you will typically be able to get your hand in beyond the knuckles. If you are flat-backed (posterior pelvic tilt), you will struggle to get the fingers in to their full depth.
In the first instance, I would expect to see the tight hip flexors, tight low back, weak hip flexors, weak glutes that I mentioned above. The best means of correcting this is with core exercise. Most hip extension exercises will typically involve the low back too and thus can serve to further train the dysfunctional pattern. Any core exercise where you are working on maintaining a neutral lordotic curve is a good exercise. I would recommend doing all of your core work either supine on the ground or with a partner holding a dowel on your back so that you can see if the curve is becoming excessive.
I guarantee, if you train your core to put your hips in the right position, your glute fibers will be in a better position to fire (at their normal resting length). When this occurs, you can begin normal glute training.
The other exercise, in addition to isometric core moves that I would recommend is prone and seated hamstring curls. Even when you do these, watch the low back though. Keep the abs on and a neutral lordotic curve throughout.
Hope this helps,
Alan Couzens, CSCS, PES, ASCA Strength and Conditioning Coach.








Did the test and found lots of room behind my back… so I gess that means I’m your example #1.
Are these the kind of exercises your talking about?
OK,
So we’ve established that you’re probably hyperlordotic which, essentially means that your low back muscle is firing more than it should. This means that your lumbar extensors will want to get involved in hip extension exercise more than they should.
So, the key for all of the exercises that you do is to make sure that you are working your glutes and inner abs *without *working your low back and outer abs.
So, looking at the exercises you provided, I’m going to put them in order of progression with a couple of guidlelines on what you should be able to do before moving to the next exercise:
-
Picture 1: Hip Flexion w/TVA contraction - You need to be able to maintain the same arch in your back throughout the exercise, i.e. when the leg is in the air, the arch should be the same as it is when you are on the ground - one handwidth, no more, no less. The best way to ascertain this is with a blood pressure cuff put under your back (trying to maintain an even pressure - 40-70mmhg throughout). Alternatively, try to keep an even pressure on your hand, i.e. back lightly pressed against your knuckles.
-
Picture 3: Prone Hip Extension. The key here is to learn the exercise with a long dowel or ruler on your back. Same rules apply, you want to maintain one handwidth between the stick and your back AT ALL TIMES (have a partner help you hold the stick and watch the curve). In the beginning it may be difficult to merely lift one knee off the ground without losing the neutral curve. As you get better though, you will be able to *slowly *extend the hip as in the picture. A more challenging version once you can do that is to do the same exercise with a straight leg.
-
Pictures 7 & 8: Crunch w/TVA contraction. Same protocol as above, doing a mini crunch without letting the back flatten out. This works the rectus abdominus and obliques in co-contraction with the TVA. Most folks with your postural distortion pattern are plenty strong in their upper abs and weak in their lower and inner abs. Therefore, it is important to work them simultaneously. When this is easy (i.e. the back is arched exactly the same throughout the crunch, you can lengthen the lever as in exercise 8.
-
Picture 9. Lower abdominal crunch. This one comes a little further down the list because the potential to cheat (and use the upper abs) is there. The key with this exercise is to go straight up, not back toward your head. Pick a dot on the ceiling directly above the feet and aim for it. Your back should maintain an arch in order to keep the legs pointing straight up. Pretty tough exercise.
-
Pictures 4&5. Hip Extension/Abduction with TVA contraction. Same rules apply as for the prone and supine exercise. Get your trusty stick out and put it behind your back and maintain a neutral curve throughout the exercise. Before even attempting this exercise, it is crucial that you can contract your abs to a neutral curve in the wall test I described in the last post. Once you can do this, try to do it standing on one leg and then you can think about moving the leg, first in a door jam and later with cable resistance as shown in the pic.
-
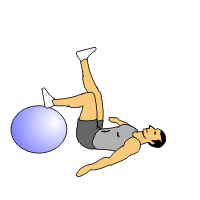
Pictures 6&2. Hip bridge/curl on a swiss ball. It is really hard to see what is getting your hips up there in this one, i.e. low back muscles v’s glutes and hamstrings. It kind of hurts to put a stick back there, so you need to be pretty confident in your ability to hold a neutral lordotic curve in all of the positions mentioned above before trying this exercise, especially on an unstable surface, like a swiss ball.
I know that this progression may seem overly cautious but it is important to remember that your low back muscles are in a much better position that your glutes to work given a chance. Therefore, if you skip a step, in all probability you are training the low back and not the glutes and propogating the dysfunctional pattern.
Hope you find this info helpful.
All the best,
Alan Couzens, CSCS, PES, ASCA Strength and Conditioning Coach.
Alan,
This is Don again. Thanks for the further insights. I did your test and my whole hand fits in the small of my back as you suggested for Paul. I appreciate your further advice and will work on these ideas as well for myself. I really appreciate your follow up on this hip flexor problem. This is more specific information than any of the providers I have been to. My PT and massage therapist are good, but do not have this depth of expertise. Slowtwitch is great. Don.
Thanks Don.
I really appreciate the kind words.
If I can help out in any way in the future, don’t hesitate to PM me.
Best regards,
Alan