Dale:
Thanks for being such a great resource.
I’m interested in your viewpoint regarding the role of statins in turning soft plaque to hard plaque; from what I’ve been able to gather, you can expect ~10% increase in your calcium score AFTER starting statins from this phenomenon.
If what we see in masters endurance athletes with elevated scores is a result of the damaged arteries calcifying (Peter Attia’s description), then I don’t follow the logic in starting a statin to see a further increase in that score.
I’ve not been able to find any evidence in the literature regarding any treatment that demonstrates a decrease in CAC scores; the only mention is anecdotal in concentration camp survivors who were starved demonstrating a reversal of CAD (of course, they weren’t doing CAC scores then). However, once they resumed a normal diet, it returned.
Jeff
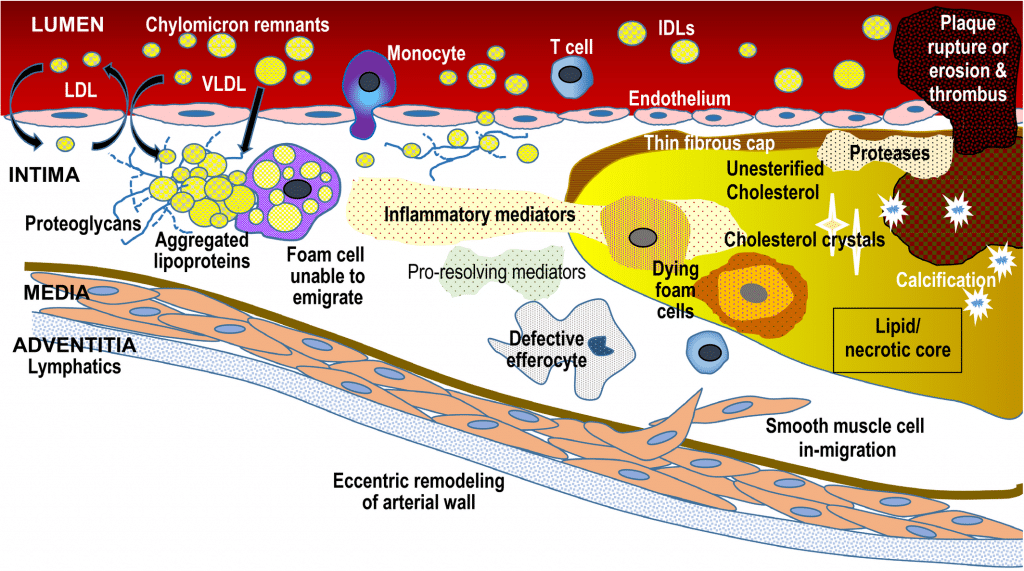
Once identified, behaviors can modify plaque and statins do exactly that-turn soft plaque *(that can become vulnerable and rupture) into hard plaque that is stable. There is increased risk with more plaque burden of all kinds, but risk actually goes down significantly when there is less soft plaque. It’s all about risk management at that point not at all about lowering your calcium score. The disease process really starts early in life and there is cumulative damage to the vessels over time made worse by so many things…
All scores will increase over time. Identifying CAD plaque and quantifying it can allow a patient to try to take better care of themselves going forward-eat better, exercise more *(if needed-although less here in the triathlon world) and for many, but not all-taking a medication to lower long term cardiac risk like a statin.
Dr. Attia is a great champion for heart disease and I enjoy his videos. He does help people learn about the disease and the process.
Talking about heart disease in general.
https://youtu.be/IbSHHESbm5U?si=1IK8Sv8WcPSSF70D
Talking about CAC
https://youtu.be/Z7MrZRInjvI?si=5VtJKzL-TAv1yQe6
CAC discussion starts ~ 1:11:00
https://youtu.be/W1geXgNEG_0?si=jKHLzr-UMEQQWGn4
I would suggest looking at the following at the science behind heart disease (coronary artery disease) and a whole food, plant-based diet. There are lots of resources out there for lay people (if that’s you) and lots of peer reviewed science if you are savvy with reading the scientific literature (pubmed). Some suggestions for where to start:
Read “prevent and reverse heart disease†by Esselstyn and/or “china study†by Campbell and/or “How not to die†by Greger
Watch “Forks over knives†documentary- streams for free on website
Watch videos/read blog on nutrition facts.org
Listen to any podcast with Kim Williams, MD
…
The leading cause of death among cardiologist is heart disease just like everyone else.
Heart disease is universal with a western diet by age 10.
“There are 2 kinds of cardiologists- vegans and those that haven’t read the scienceâ€
All adults should consume a healthy diet that emphasizes the intake of vegetables, fruits, nuts, whole grains, lean vegetable or animal protein, and fish and minimizes the intake of trans fats, red meat and processed red meats, refined carbohydrates, and sweetened beverages. For adults with overweight and obesity, counseling and caloric restriction are recommended for achieving and maintaining weight loss.
Everyone should absolutely understand that any non- heart healthy diet is very significantly contributory to CAD and soft plaque formation. There is no argument from me that plant based, dash, ornish and mediterranean diets all are much better than most western diets. But diet can only lower risk by about 15%. Statins work adjunctively with diet to lower risk and actually work far better absolutely.
And it is awfully difficult to modify patients behavior-especially eating. People do like to eat…
-
LDL isn’t the best metric for identification of heart disease, it’s actually the number of LP(a) particles as the primary driver. Amgen has a drug in a clinical trial to reduce LP(a) and thus slow the progression of coronary artery disease (CAD). I don’t want to get too technical here, so here’s a link about it if you want to read up: https://www.amgen.com/...w-about-lipoproteina
-
PSK9 Inhibitors is the only treatment know to reduce LP(a) concentration, but most insurance won’t pay for it, so the best alternative option is a statin that reduces your total LDL number. Interestingly, statins increase the LP(a) concentration; however, this risk is overwhelmed by the benefit of total LDL decrease. For what it’s worth, my cardiologist has me on 40mg of Rouvastatin and 10mg of Ezetimibe to keep my LDL under 70. And yes, I take CoQ10 to offset muscle fatigue.
-
People who exercise generally have better plaque composition. There’s a ton of research in this area using athletes over age 50, but my takeaway was the process of exercise functions similar to a statin in that it turns soft plaque into a safer denser plaque. It’s the dense plaque that gets shown in your calcium score, not the soft plaque, so ironically people with a lower calcium can in some cases be at more risk. Lastly, athletes tend to build collateral pathways to promote blood flow leading to my next finding.
-
Stress test results and METS achieved have prognostic charts similar to calcium score charts. Based on my calcium score, I was in the bottom 5% with the highest risk. Based on my stress test, I’m at the top 5% with the lowest risk.
Overall, I think there’s A LOT still being learned about CAD in athletes, but exercise serves as a protective mechanism which could enable us to live to be 100 years old with arteries full of dense calcium. Perhaps even taking a statin is redundant and unnecessary, but we aren’t far enough along our learning cycle to say that with confidence. It sucks that you were dealt a bad hand, but realize it’s not all gloom and doom. Just keep doing what you enjoy and follow your cardiologist’s advice to slow the progression of the disease and calcify the soft plague. Good luck!
I think there is always more to learn about CAD. But once risk is identified, there are coronary vessels that have plaque and taking a statin is the BEST known treatment for mitigating risk. Once treated and at lower risk, progression is slowed and plaque becomes more stable. Then you can not only enjoy exercise but also know there is truly lower risk. And I’d say were are certainly far along enough to say that confidently.
Stress tests are done to evaluate whether there is elevated risk from a physiologic standpoint. Is there a significant blockage causing EKG changes suggesting higher risk? You can certainly have higher or lower risk with elevated coronary scores and that’s why patients with high numbers get additional testing to re-classify risk.
I also agree that Lp(a) and ApoB are truly important and help identify risk. We are still learning the best way to treat elevated numbers for these. This may be a bit busy, but perhaps helpful to some.