NealH wrote:
It takes about a month. No big deal.Triathlon Forum
Login required to started new threads
Login required to post replies
Re: Atrial fibrillation as a athlete. [NealH]
[ In reply to ]
My experience was about the same, FWIW.
Re: Atrial fibrillation as a athlete. [Soarfeet]
[ In reply to ]
Soarfeet - I looked through my data but don't have anything in Garmin for just post-ablation. Mine was 10/2014, I do have data from 2015 that I was well into training again by spring and racing by August at the very least. But I highly doubt I was doing anything intense for the first month, given my recollection of general chest tightness and lethargy.
Re: Atrial fibrillation as a athlete. [LDF]
[ In reply to ]
LDF wrote:
Just curious, I had my ablation last Wednesday (4/13) and since then my resting HR has been elevated by about 20-25 bpm. My Dr. warned me that might be the case, but I wanted to see if anyone here had a similar "side effect" and if so, for how long? Thanks!Mine actually went down immediately. My resting HR had been a bit higher for a few years just before afib hit, in the upper 40s, then was anywhere from 75-220 for the 8 months until I had the ablation. While in the hospital recovering from the ablation, it was at 42, where it had been until about 5 years earlier...
"I'm thinking of a number between 1 and 10, and I don't know why!"
Re: Atrial fibrillation as a athlete. [Kirch]
[ In reply to ]
Hello Kirch and All,
My wife has Afib occasionally even though she has had an ablation ... everything fine for 3 or 4 months and then has an episode that may last 2 days ... her age is 86
She has a Biotronik pacemaker and takes some drugs to prevent Afib along with Warfarin to reduce possible clotting.
There is a procedure ... whereby using a device that can externally control the Biotronik pacemaker ... the operator can run her pulse up to 250 and right back down and it will stop the Afib.
The Biotroik tech says the procedure only works on 60% or so of patients .. but is is magic when Afib occurs .. and we can get to the doctor's office.
I also have a Biotronik pacemaker because my heart rate was skipping as I aged at a normal resting pulse of 42 .. a double skip would result in a loss of consciousness. The Biotronik keeps heart rate floor at 50 now.
My age will be 90 next year ... The Biotronic pacemaker has a device like a cell phone next to the bed that (Bluetooth?) collects and sends the downloaded file of heartbeats stored each day in the Biotronik via the bedside device selfcontained cellphone to my cardiologist each day with
anomalies flagged.
Recently, after several years with the Biotronik, I had my first Afib event (I was unaware of it) and was called in for some tests and started Warfarin to prevent blood clots in the future.
Today I discussed getting a Watchman installed in my heart and not taking Warfarin in the future. I was told that the procedure takes about an hour and although I was old, I was otherwise very healthy and it should be possible.
Cheers, Neal
+1 mph Faster
My wife has Afib occasionally even though she has had an ablation ... everything fine for 3 or 4 months and then has an episode that may last 2 days ... her age is 86
She has a Biotronik pacemaker and takes some drugs to prevent Afib along with Warfarin to reduce possible clotting.
There is a procedure ... whereby using a device that can externally control the Biotronik pacemaker ... the operator can run her pulse up to 250 and right back down and it will stop the Afib.
The Biotroik tech says the procedure only works on 60% or so of patients .. but is is magic when Afib occurs .. and we can get to the doctor's office.
I also have a Biotronik pacemaker because my heart rate was skipping as I aged at a normal resting pulse of 42 .. a double skip would result in a loss of consciousness. The Biotronik keeps heart rate floor at 50 now.
My age will be 90 next year ... The Biotronic pacemaker has a device like a cell phone next to the bed that (Bluetooth?) collects and sends the downloaded file of heartbeats stored each day in the Biotronik via the bedside device selfcontained cellphone to my cardiologist each day with
anomalies flagged.
Recently, after several years with the Biotronik, I had my first Afib event (I was unaware of it) and was called in for some tests and started Warfarin to prevent blood clots in the future.
Today I discussed getting a Watchman installed in my heart and not taking Warfarin in the future. I was told that the procedure takes about an hour and although I was old, I was otherwise very healthy and it should be possible.
Cheers, Neal
+1 mph Faster
Re: Atrial fibrillation as a athlete
[ In reply to ]
Hi everyone,
Recently my doctor prescribed a holter monitor which indicates mild arrythmia (something ventricular tachycardia?) that starts and lasts about 5 beats. I thought I just consumed too much caffeine and or had anxiety.......
I am awaiting an echocardiogram. My research indicates that this is common with athletes, especially those who have been endurance athletes for years like me. Does anyone have experience training and or racing with this? My doctor has said no worries exercising as long as I don't exhibit additional symptoms (ie. passing out, etc.). I am anxiously waiting for the eco test and an appointment with a cardiologist. I do not exhibit extremely high heart rate episodes while exercising (or at least not that I know of).....
Thanks!
KK
Recently my doctor prescribed a holter monitor which indicates mild arrythmia (something ventricular tachycardia?) that starts and lasts about 5 beats. I thought I just consumed too much caffeine and or had anxiety.......
I am awaiting an echocardiogram. My research indicates that this is common with athletes, especially those who have been endurance athletes for years like me. Does anyone have experience training and or racing with this? My doctor has said no worries exercising as long as I don't exhibit additional symptoms (ie. passing out, etc.). I am anxiously waiting for the eco test and an appointment with a cardiologist. I do not exhibit extremely high heart rate episodes while exercising (or at least not that I know of).....
Thanks!
KK
Re: Atrial fibrillation as a athlete. [Kirch]
[ In reply to ]
I responded to the afib inquiry in another thread, but it is not linked so I copied most of the important stuff.
As always, discuss your own situation with your MD-the internet is not where you should get your medical information. It is well known and documented that afib is associated with activity/exercise.
When afib is discovered (new), we have to decide if it is a triggered issue or not. Meaning, was the reason the heart rhythm going out of rhythm just trouble with the electrical system or if it was caused by an irritant like: alcohol, hormones-like an overactive thyroid, dehydration, severe anemia, or other systemic disease which may or may not be known-especially heart disease. It can be caused by exercise and emotional stress also. The biggest concern is undiagnosed heart disease.
It may come and go (paroxysmal) or become persistent>permanent. There are ways to put the heart rhythm back to normal-with electricity or medication. Some people will need to be on blood thinners/anti-coagulants (AC). The first decision for new afib is to figure out why it happened. Labs and some cardiac testing is usually needed because cardiac disease is the most common underlying concern. Decisions are made based on a decision to either rate control or rhythm control-put the patient back into sinus rhythm. Most patients have very rapid rates when in new afib and are symptomatic.
Some HR monitors are pretty accurate. A lot of the ones with optical sensors are pretty inaccurate but give some useful information at times.The apple watch isn't too bad either but it's not perfect, for sure. Monitors using a chest strap are much more accurate but still not perfect. Movement can mimic afib by artifact. A Kardia device is a much better and more accurate device for checking for afib. The Kardia is worth the $99 bucks and can be uploaded and delivered to an MD for review. Symptoms have to be occurring long enough to get your fingers on the device, though.
One of the risks of doing exercise with very rapid afib is syncope as the heart is going much too fast to fill and pump efficiently so BP can dive and that can be followed by the patient hitting the deck. Something additionally to think about...
-----------------------------------------------------------------------------------
Up To Date has a nice 'summary' about afib-see some of it below which I cut/pasted/added.
Overview of atrial fibrillation
INTRODUCTION
Atrial fibrillation (AF) is the most commonly treated cardiac arrhythmia.
AF is generally associated with an irregularly irregular ventricular rhythm and absence of distinct P waves.
Complications of AF include risk of thromboembolism (including stroke) and risk of heart failure. In addition, affected patients may be at increased risk for mortality.
PREVALENCE AND ASSOCIATED CONDITIONS
The prevalence of AF increases with age, and it is estimated to affect over 4 percent of the population above the age of 60. Hypertensive heart disease and coronary heart disease are the most common underlying disorders in patients with AF in developed countries. Rheumatic heart disease is prevalent in certain resource-limited areas and is strongly associated with AF.
●Associated conditions – Hypertensive heart disease and coronary heart disease are the most common underlying disorders associated with AF in developed countries. It also occurs with cardiomyopathy and heart valve disease.
It also occurs in athletes-especially endurance athletes.
CLASSIFICATION
AF is classified according to the following schema described in the 2014 American Heart Association/American College of Cardiology/Heart Rhythm Society guidelines on AF management
●Paroxysmal (ie, self-terminating or intermittent) AF – Paroxysmal AF is defined as AF that terminates spontaneously or with intervention within seven days of onset. Episodes may recur with variable frequency. (See "Paroxysmal atrial fibrillation".)
●Persistent AF – Persistent AF is defined as AF that fails to self-terminate within seven days. Episodes often require pharmacologic or electrical cardioversion to restore sinus rhythm. While a patient who has had persistent AF can have later episodes of paroxysmal AF, AF is generally considered a progressive disease.
●Long-standing persistent AF – Long-standing persistent AF refers to AF that has lasted for more than 12 months.
●Permanent AF – Permanent AF is a term used to identify persistent AF for which a joint decision by the patient and clinician has been made to no longer pursue a rhythm control strategy. Acceptance of persistent AF may change as symptoms, therapeutic options, and patient and clinician preferences evolve.
While AF typically progresses from paroxysmal to persistent states, patients can present with both types throughout their lives.
The term "lone AF" is a historical term that is now disfavored as it may be confusing and does not enhance patient care. The term lone AF has been used to describe AF in younger patients (eg, ≤60 years) with paroxysmal, persistent, or permanent AF who have no structural heart disease or cardiovascular risk factors. These characteristics identify a group of individuals with a CHA2DS2-VASc score of "0" and are lowest risk of thromboembolism from AF.
Subclinical AF (SCAF) is defined as episodes of AF detected by intracardiac, implantable, or wearable monitors and confirmed by intracardiac electrogram or review of the recorded rhythm on the electrocardiogram (ECG). SCAF usually occurs in individuals without characteristic symptoms of AF and without a prior diagnosis. Most of these individuals will have paroxysmal AF. A scientific statement from the American Heart Association on subclinical and device-detected AF was published in 2019.
The prevalence of SCAF depends on the population studied as well as the duration, sensitivity, and specificity of screening techniques. The following studies investigated the prevalence of subclinical AF in different populations, using different monitoring techniques:
●In the STROKESTOP observational study of 7173 individuals 75 to 76 years of age in Sweden, previously unknown AF was detected using intermittent ECG recordings over three weeks in 3 percent.
●The ASSERT study monitored (using a dual-chamber pacemaker or implantable cardioverter defibrillator) 2580 patients (65 years or older) with hypertension and no history of AF for the development of AF (defined as episodes of atrial rate >190 beats per minute for more than six minutes). The following findings were noted:
•At three months, subclinical AF was detected in about 10 percent of patients. The median number of episodes was two, and the median time to detection of the first episode was 36 days.
•At 2.5 years, SCAF was detected in about 35 percent of individuals. Clinical AF developed in about 16 percent of patients with SCAF.
●In the ASSERT-II study of 256 patients (mean age of 74 years; mean CHA2DS2-VASc score of 4.1) with an implanted subcutaneous ECG monitor who were followed for about 16 months, one or more episodes of SCAF lasting ≥5 minutes occurred in 34 percent. This was a high-risk population, as 48 percent (of the 256 patients) had prior stroke, transient ischemic attack, or systemic embolism.
●In a study of 590 individuals with stroke risk factors but without AF who underwent screening with an implantable loop recorder for an average of 40 months, 35 percent of participants were found to have AF.
AFib can kill you but most often is just irritating -initially, but over time there is increased risk.
Electrocardiogram — In AF, there are no discrete P waves but rapid, low-amplitude, continuously varying fibrillatory (f) waves are seen. The ventricular rhythm is generally irregularly irregular (lacking a repetitive pattern), although AF is uncommonly associated with a regular ventricular rate. The ECG in patients with AF is described in detail separately. (See "The electrocardiogram in atrial fibrillation".)
There are a number of potential pitfalls in the ECG diagnosis of AF. Errors in the diagnosis of AF are especially common with computerized ECG interpretation and in patients who are continuously or intermittently paced. Hence, it is important that the automated ECG interpretation provided by the machine is confirmed by a skilled reader

MANAGEMENT
A useful framework for the general care of AF patients is the ABC (Atrial Fibrillation Better Care) pathway. The "A" can be considered for anticoagulation, "B" for better symptom management, and "C" for cardiovascular risk factor and comorbid disease assessment and management. Mitigating the risk of stroke is one of the most important management considerations for physicians treating AF patients, and the long-term use of oral anticoagulants is the most effective means of reducing risk of stroke. However, the risk of stroke must be weighed against the risk of bleeding from these anticoagulants with the use of such scores as CHA2DS2-VASc and HAS-BLED. Symptom management starts with rate control of acute AF episodes and then extends to assessment of the benefits of rhythm control over the longer term. Finally, identifying and treating risk factors and comorbidities, such as obesity, sleep apnea, hypertension, and heart failure, may help with AF symptoms and burden. Observational studies, a post-hoc analysis of the AFFIRM trial, and a prospective randomized trial using a mobile application suggest that the implementation of such a framework of care for AF patients may have a salutary impact on adverse cardiovascular events and hospitalizations, while being cost saving for healthcare systems.
Healthcare providers are presented with two broad types of patients with AF: those with newly diagnosed AF and those who have been previously diagnosed and managed. Care of the former includes decisions regarding the need for anticoagulation and the choice between rate or rhythm control strategies. For patients with established diagnosis, periodic assessment of the adequacy of treatment is necessary.
Link to the CHADSVASC and HASBLED scoring calculators.
CHADSVASC, CHA2DS2VASC and HASBLED risk score calculator for atrial fibrillation
Many patients will need cardiac evaluation to look for ischemic heart disease, valve disease or cardiomyopathy. Testing may include a coronary artery calcium score, cardiac echo or stress test.
Cardioversions work to restore sinus rhythm pretty well (~90% success initially), for a time, and can be done repeatedly. With recurrences, ablation is a better long term solution but there are risks also

edited to add Dr. Creswell's blog from long ago as he is more succinct with words than I am
Atrial Fibrillation in Athletes (In a Nutshell) (athletesheart.org)
Also forgot to mention the Watchman Device, which our hospital and many others do put in-if eligible
WATCHMAN Implant for Non-Valvular Afib Stroke Risk
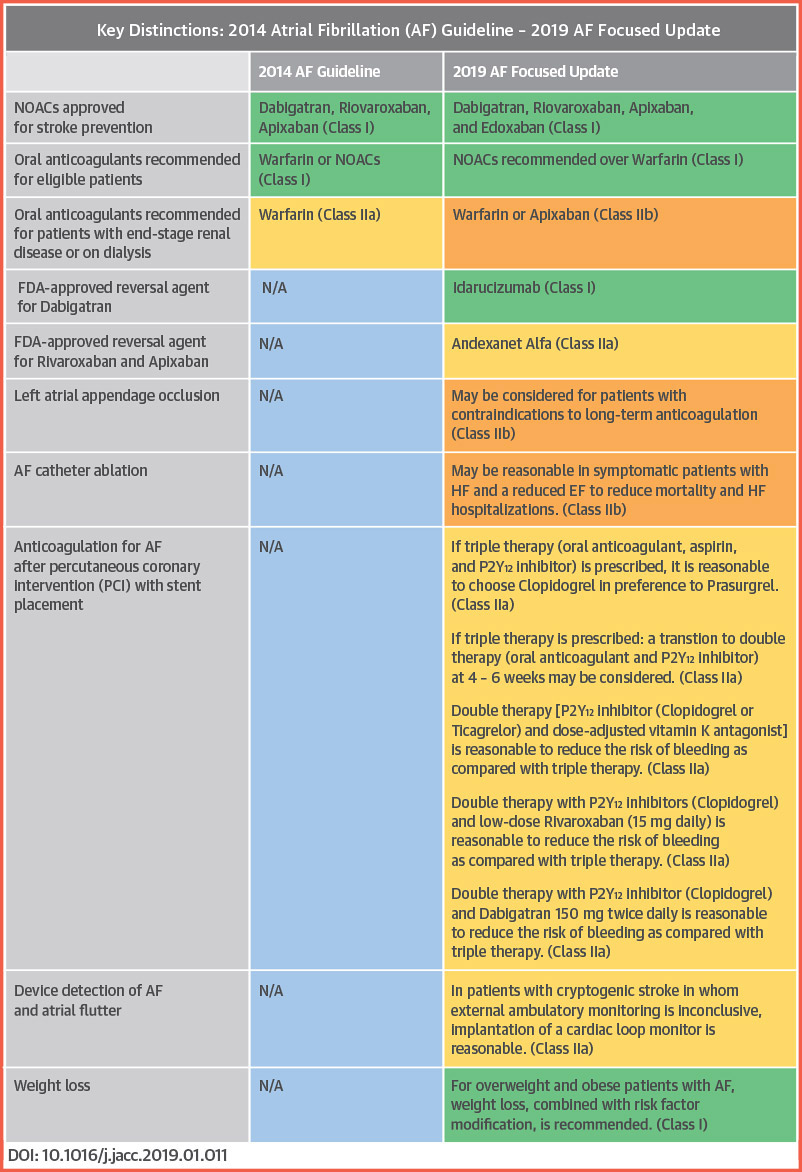
Updated Rx guidelines
Hope this helps.
As always, discuss your own situation with your MD-the internet is not where you should get your medical information. It is well known and documented that afib is associated with activity/exercise.
When afib is discovered (new), we have to decide if it is a triggered issue or not. Meaning, was the reason the heart rhythm going out of rhythm just trouble with the electrical system or if it was caused by an irritant like: alcohol, hormones-like an overactive thyroid, dehydration, severe anemia, or other systemic disease which may or may not be known-especially heart disease. It can be caused by exercise and emotional stress also. The biggest concern is undiagnosed heart disease.
It may come and go (paroxysmal) or become persistent>permanent. There are ways to put the heart rhythm back to normal-with electricity or medication. Some people will need to be on blood thinners/anti-coagulants (AC). The first decision for new afib is to figure out why it happened. Labs and some cardiac testing is usually needed because cardiac disease is the most common underlying concern. Decisions are made based on a decision to either rate control or rhythm control-put the patient back into sinus rhythm. Most patients have very rapid rates when in new afib and are symptomatic.
Some HR monitors are pretty accurate. A lot of the ones with optical sensors are pretty inaccurate but give some useful information at times.The apple watch isn't too bad either but it's not perfect, for sure. Monitors using a chest strap are much more accurate but still not perfect. Movement can mimic afib by artifact. A Kardia device is a much better and more accurate device for checking for afib. The Kardia is worth the $99 bucks and can be uploaded and delivered to an MD for review. Symptoms have to be occurring long enough to get your fingers on the device, though.
One of the risks of doing exercise with very rapid afib is syncope as the heart is going much too fast to fill and pump efficiently so BP can dive and that can be followed by the patient hitting the deck. Something additionally to think about...
-----------------------------------------------------------------------------------
Up To Date has a nice 'summary' about afib-see some of it below which I cut/pasted/added.
Overview of atrial fibrillation
INTRODUCTION
Atrial fibrillation (AF) is the most commonly treated cardiac arrhythmia.
AF is generally associated with an irregularly irregular ventricular rhythm and absence of distinct P waves.
Complications of AF include risk of thromboembolism (including stroke) and risk of heart failure. In addition, affected patients may be at increased risk for mortality.
PREVALENCE AND ASSOCIATED CONDITIONS
The prevalence of AF increases with age, and it is estimated to affect over 4 percent of the population above the age of 60. Hypertensive heart disease and coronary heart disease are the most common underlying disorders in patients with AF in developed countries. Rheumatic heart disease is prevalent in certain resource-limited areas and is strongly associated with AF.
●Associated conditions – Hypertensive heart disease and coronary heart disease are the most common underlying disorders associated with AF in developed countries. It also occurs with cardiomyopathy and heart valve disease.
It also occurs in athletes-especially endurance athletes.
CLASSIFICATION
AF is classified according to the following schema described in the 2014 American Heart Association/American College of Cardiology/Heart Rhythm Society guidelines on AF management
●Paroxysmal (ie, self-terminating or intermittent) AF – Paroxysmal AF is defined as AF that terminates spontaneously or with intervention within seven days of onset. Episodes may recur with variable frequency. (See "Paroxysmal atrial fibrillation".)
●Persistent AF – Persistent AF is defined as AF that fails to self-terminate within seven days. Episodes often require pharmacologic or electrical cardioversion to restore sinus rhythm. While a patient who has had persistent AF can have later episodes of paroxysmal AF, AF is generally considered a progressive disease.
●Long-standing persistent AF – Long-standing persistent AF refers to AF that has lasted for more than 12 months.
●Permanent AF – Permanent AF is a term used to identify persistent AF for which a joint decision by the patient and clinician has been made to no longer pursue a rhythm control strategy. Acceptance of persistent AF may change as symptoms, therapeutic options, and patient and clinician preferences evolve.
While AF typically progresses from paroxysmal to persistent states, patients can present with both types throughout their lives.
The term "lone AF" is a historical term that is now disfavored as it may be confusing and does not enhance patient care. The term lone AF has been used to describe AF in younger patients (eg, ≤60 years) with paroxysmal, persistent, or permanent AF who have no structural heart disease or cardiovascular risk factors. These characteristics identify a group of individuals with a CHA2DS2-VASc score of "0" and are lowest risk of thromboembolism from AF.
Subclinical AF (SCAF) is defined as episodes of AF detected by intracardiac, implantable, or wearable monitors and confirmed by intracardiac electrogram or review of the recorded rhythm on the electrocardiogram (ECG). SCAF usually occurs in individuals without characteristic symptoms of AF and without a prior diagnosis. Most of these individuals will have paroxysmal AF. A scientific statement from the American Heart Association on subclinical and device-detected AF was published in 2019.
The prevalence of SCAF depends on the population studied as well as the duration, sensitivity, and specificity of screening techniques. The following studies investigated the prevalence of subclinical AF in different populations, using different monitoring techniques:
●In the STROKESTOP observational study of 7173 individuals 75 to 76 years of age in Sweden, previously unknown AF was detected using intermittent ECG recordings over three weeks in 3 percent.
●The ASSERT study monitored (using a dual-chamber pacemaker or implantable cardioverter defibrillator) 2580 patients (65 years or older) with hypertension and no history of AF for the development of AF (defined as episodes of atrial rate >190 beats per minute for more than six minutes). The following findings were noted:
•At three months, subclinical AF was detected in about 10 percent of patients. The median number of episodes was two, and the median time to detection of the first episode was 36 days.
•At 2.5 years, SCAF was detected in about 35 percent of individuals. Clinical AF developed in about 16 percent of patients with SCAF.
●In the ASSERT-II study of 256 patients (mean age of 74 years; mean CHA2DS2-VASc score of 4.1) with an implanted subcutaneous ECG monitor who were followed for about 16 months, one or more episodes of SCAF lasting ≥5 minutes occurred in 34 percent. This was a high-risk population, as 48 percent (of the 256 patients) had prior stroke, transient ischemic attack, or systemic embolism.
●In a study of 590 individuals with stroke risk factors but without AF who underwent screening with an implantable loop recorder for an average of 40 months, 35 percent of participants were found to have AF.
AFib can kill you but most often is just irritating -initially, but over time there is increased risk.
Electrocardiogram — In AF, there are no discrete P waves but rapid, low-amplitude, continuously varying fibrillatory (f) waves are seen. The ventricular rhythm is generally irregularly irregular (lacking a repetitive pattern), although AF is uncommonly associated with a regular ventricular rate. The ECG in patients with AF is described in detail separately. (See "The electrocardiogram in atrial fibrillation".)
There are a number of potential pitfalls in the ECG diagnosis of AF. Errors in the diagnosis of AF are especially common with computerized ECG interpretation and in patients who are continuously or intermittently paced. Hence, it is important that the automated ECG interpretation provided by the machine is confirmed by a skilled reader

MANAGEMENT
A useful framework for the general care of AF patients is the ABC (Atrial Fibrillation Better Care) pathway. The "A" can be considered for anticoagulation, "B" for better symptom management, and "C" for cardiovascular risk factor and comorbid disease assessment and management. Mitigating the risk of stroke is one of the most important management considerations for physicians treating AF patients, and the long-term use of oral anticoagulants is the most effective means of reducing risk of stroke. However, the risk of stroke must be weighed against the risk of bleeding from these anticoagulants with the use of such scores as CHA2DS2-VASc and HAS-BLED. Symptom management starts with rate control of acute AF episodes and then extends to assessment of the benefits of rhythm control over the longer term. Finally, identifying and treating risk factors and comorbidities, such as obesity, sleep apnea, hypertension, and heart failure, may help with AF symptoms and burden. Observational studies, a post-hoc analysis of the AFFIRM trial, and a prospective randomized trial using a mobile application suggest that the implementation of such a framework of care for AF patients may have a salutary impact on adverse cardiovascular events and hospitalizations, while being cost saving for healthcare systems.
Healthcare providers are presented with two broad types of patients with AF: those with newly diagnosed AF and those who have been previously diagnosed and managed. Care of the former includes decisions regarding the need for anticoagulation and the choice between rate or rhythm control strategies. For patients with established diagnosis, periodic assessment of the adequacy of treatment is necessary.
Link to the CHADSVASC and HASBLED scoring calculators.
CHADSVASC, CHA2DS2VASC and HASBLED risk score calculator for atrial fibrillation
Many patients will need cardiac evaluation to look for ischemic heart disease, valve disease or cardiomyopathy. Testing may include a coronary artery calcium score, cardiac echo or stress test.
Cardioversions work to restore sinus rhythm pretty well (~90% success initially), for a time, and can be done repeatedly. With recurrences, ablation is a better long term solution but there are risks also
edited to add Dr. Creswell's blog from long ago as he is more succinct with words than I am
Atrial Fibrillation in Athletes (In a Nutshell) (athletesheart.org)
Also forgot to mention the Watchman Device, which our hospital and many others do put in-if eligible
WATCHMAN Implant for Non-Valvular Afib Stroke Risk
Updated Rx guidelines
Hope this helps.
Re: Atrial fibrillation as a athlete. [dtoce]
[ In reply to ]
https://www.upi.com/...rinks/3061709629717/
I happen to see the above and thought of this thread I can’t remember if I was drinking diet soda when I had my afib but I believe I was drinking quite a bit
Fortunately by happenstance I no longer drink it at all.
Completely separate here is an update to my situation I posted about up above back in 2022
Coranary calcium score. Great. Stress test great. All other tests great
Happy to say never went into afib again
Started on 2 tablespoon of flax every day. Within 6 weeks Blood pressure routinely at 117/72. And has been that was for a year
No more anxiety
Pounding heart, NOT fast but sometimes BOOM BOOM BOOM for up to an hour or 2 continued until 6 months ago when I started magnesium supplements AM and PM. If I sleep a couple days the BOOM comes back.
So now No more pounding heart
happy to say no more anxiety,
Still wake 5 - 8 times per night to roll over and quickly go back to sleep
routinely get 8.5 - 9.5 hours of sleep
Back to full training.
Blood tests take. Last week all perfect except HDL cholesterol is 107. BUT ratio is great and threat of cardiac problems low
Of course super happy with the results
I happen to see the above and thought of this thread I can’t remember if I was drinking diet soda when I had my afib but I believe I was drinking quite a bit
Fortunately by happenstance I no longer drink it at all.
Completely separate here is an update to my situation I posted about up above back in 2022
Coranary calcium score. Great. Stress test great. All other tests great
Happy to say never went into afib again
Started on 2 tablespoon of flax every day. Within 6 weeks Blood pressure routinely at 117/72. And has been that was for a year
No more anxiety
Pounding heart, NOT fast but sometimes BOOM BOOM BOOM for up to an hour or 2 continued until 6 months ago when I started magnesium supplements AM and PM. If I sleep a couple days the BOOM comes back.
So now No more pounding heart
happy to say no more anxiety,
Still wake 5 - 8 times per night to roll over and quickly go back to sleep
routinely get 8.5 - 9.5 hours of sleep
Back to full training.
Blood tests take. Last week all perfect except HDL cholesterol is 107. BUT ratio is great and threat of cardiac problems low
Of course super happy with the results
To add some another data point. I'm currently 30 years old and I just came out of a PVI ablation yesterday. I've swam competivitely for 12 years and raced bikes for for 10. I started exhibiting afib when I was ~28 years old with suspected first incidents around 26 years old. I do have some family history with a relative also having afib.
My afib is relatively well controlled occurring for a few hours about every week with heart rate never going above 90 bpm during afib, and dofetilide (needs 3 days hospital admissions was above to turn most of those incidents into skipped beats.
I figured I should get the ablation done sooner rather than later as success rates are higher the earlier you do it. One day out of surgery my resting heart rate is about 15 beats higher than normal, but I was told that is to be expected.
My afib is relatively well controlled occurring for a few hours about every week with heart rate never going above 90 bpm during afib, and dofetilide (needs 3 days hospital admissions was above to turn most of those incidents into skipped beats.
I figured I should get the ablation done sooner rather than later as success rates are higher the earlier you do it. One day out of surgery my resting heart rate is about 15 beats higher than normal, but I was told that is to be expected.